


MAINE, USA — In 2021, the Legislature’s government oversight committee directed the state watchdog agency to investigate the deaths of four children whose families had some involvement with the child welfare system.
On Wednesday, the Office of Program Evaluation and Government Accountability presented the last of its four reports, this one on the death of 1-month-old Sylus Melvin.
The report found the caseworker was thorough and the steps taken met agency standards based on what was known at the time. But like the others before it, the report did little to answer the legislators’ most important question: What could the office have done differently to prevent the tragedy?
Three years and countless investigative hours later, answers remain elusive.
During Wednesday’s hearing, Sen. Jeff Timberlake, R-Turner, asked the Office of Child and Family Services director, Bobbi Johnson, “What would you do different today that didn’t happen?”
Johnson said the question “was a hard one.”
“The cases that we are involved with are complex,” Johnson said before explaining that any death weighs heavily on her staff, who “feel a huge responsibility” for “protecting children in our state.”
As in OPEGA’s report, Johnson concluded that “this caseworker did the things that we would have asked her to do.”
The OPEGA reports, released over an 18-month span, examined department actions leading up to the deaths of Hailey Goding, Maddox Williams, Jaden Harding and Sylus Melvin. OPEGA explained it judged those actions “in light of prevailing child protection policy and practice, the laws governing such matters, and the information known (or that should have reasonably been known) to authorities when the decisions were made.”
In two of the cases, it did not find that any decision involving the safety of the children was “unsound.” In a third case, OPEGA found “unsound safety decisions,” but they were both related to people in and around the home of the child, none of whom were involved in the child’s death. In the fourth case, OPEGA found the casework was “sound” and caseworker efforts were “thorough.”
The reports are just some of the many Maine has solicited on its embattled child welfare system. The state has spent at least $1.6 million on such reviews in recent years, the Bangor Daily News reported in July.
Here are takeaways from the four reports:
Hailey Goding
OPEGA “did not conclude that any OCFS decisions regarding Hailey Goding were unsound,” the agency wrote in its report on the case.
The 3-year-old Goding died from exposure to fentanyl at her Old Town home in 2021. Her mother pleaded guilty to manslaughter and is serving a 26-year prison sentence, with all but 19 suspended.
The OPEGA report notes that in May 2020, Hillary Goding, the subject of previous reports to the department, brought her daughter Hailey to a hospital emergency department.
Goding said Hailey picked up a piece of tinfoil and put it in her mouth, which Goding believed had substances on it. Shortly after, Hailey started falling asleep at the playground, prompting Goding to bring the girl to the emergency room. The report notes that at the hospital Goding appeared to be acting “appropriate” and “not under the influence of any substances.”
Hailey tested positive for cocaine at the hospital, which did not have the ability to test for fentanyl. The mother and daughter were sent to a second hospital, where they both tested positive for fentanyl. Goding denied having used, and said she might have tested positive because she touched the tinfoil in Hailey’s mouth.
Child welfare workers were immediately suspicious of Goding’s story, and believed her daughter likely ingested drugs in Goding’s possession, not found on a playground. But they were limited in their ability to seek a court-ordered removal of Hailey from her mother’s care, mainly by the account of a local school district employee who “completely corroborated” Goding’s story about what occurred on the playground.
In addition, “there were well-established fears and beliefs within child protective services and other first responder communities of fentanyl exposure through only incidental skin contact, and Ms. Goding’s assertion was accepted as possible,” OPEGA wrote.
Instead of seeking to remove Hailey from Goding’s care, the department developed a safety plan. It included making sure there was “a second caregiver” in the home, Goding would participate “in random, observed drug screens,” and not possess, use or expose Hailey to illicit substances or people who use them. The plan also required that Goding participate in mental health and substance abuse counseling, the report said.
The case closed in July with no findings of abuse or neglect and the family was moved to an alternative response program to continue services. But despite her efforts, Goding was unable to get into therapy, the report said.
By October, the alternative response program “learned that there had still been no response from the therapy referral, and Ms. Goding and the case manager were looking into other therapy options. The ARP service case was closed.”
Hailey died from fentanyl exposure the following June.
In its report, OPEGA pointed to the need to improve access to services: “Mental health, trauma, and substance abuse treatment counseling; parenting and daily living skills classes; and batterer’s intervention programs all appear to be commonly recommended services. However, from our work on this case and other child protective services reviews, we understand that there is a pronounced lack of available services that may vary based on the geographic location or the specific type of service sought.”
The agency also recommended that the office establish a central resource for substance-related questions, noting that “establishing such a resource would be beneficial to caseworkers in the future as they encounter various drug-related scenarios and may have questions about certain exposures, interactions and presentations that may ultimately impact safety decisions.”
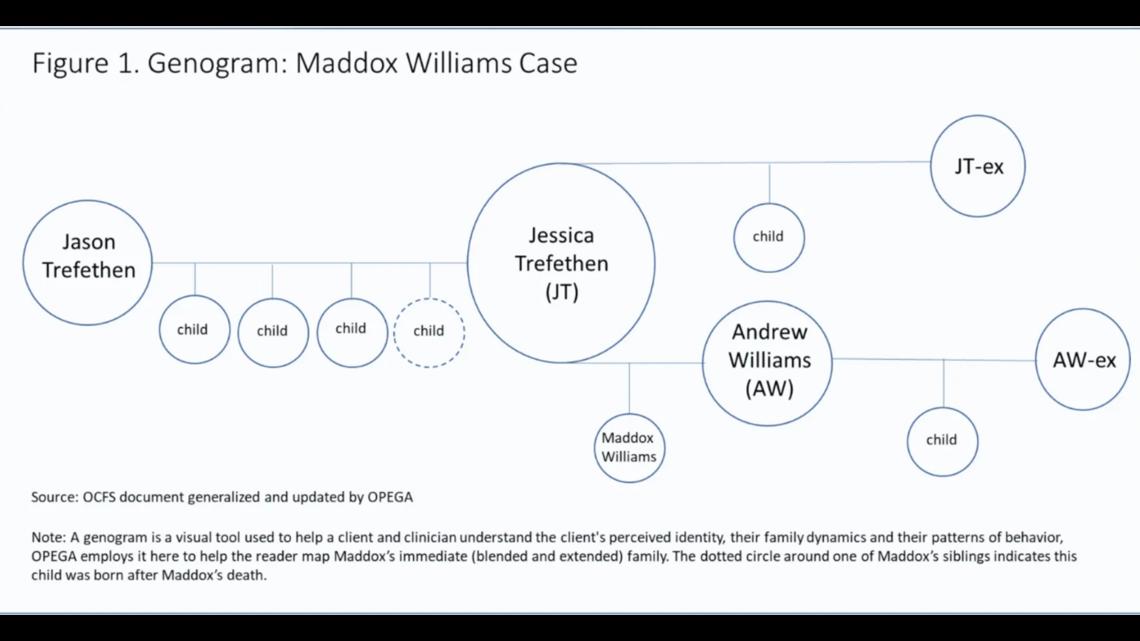
Maddox Williams
Three-year-old Maddox Williams was beaten to death by his mother Jessica Trefethen in June 2021. She was convicted of depraved indifference murder.
OPEGA “concluded that OCFS safety decisions regarding Maddox Williams were not unsound.”
The report explained that OCFS had a long history of involvement with Trefethen and her children, including Maddox, the one child born to Trefethen during a separation from her partner. But for Trefethen, most of OCFS involvement was drug-related and resulted in his living with his father for a time, before the father was found to have been driving drunk with Maddox and another child in his car.
There was nothing in the record to suggest she was a physical threat to her children, the report said.
“Trefethen was an alleged victim – not an alleged perpetrator – of domestic violence,” the report noted. During all her years with OCFS, a caseworker never found, or was provided evidence, that she “posed a threat of physical abuse to her children.”
In addition, she was “compliant with her medicated-assisted treatment program.”
In April, a caseworker visited Trefethen’s home after she called 911 as an alleged victim of domestic violence by her partner. Shortly after, a caseworker visited the home and saw Maddox sleeping with “no marks, bruises or injuries … observed on the uncovered parts of either child.”
Maddox was killed two months later.
In its report, OPEGA recommended that OCFS update its training sessions and policies to encourage caseworkers to fully explore custodial arrangements: “Understanding the composition of the household, including any out-of-home parents and the corresponding custodial arrangements (such as when the child will be residing with the other parent), may be a means of obtaining information about the family, and the potential risk and safety concerns.”

The agency noted that the scope of the OCFS investigation was limited to the most significant risks and individuals, “rather than serving as an exhaustive, comprehensive review of all potential risk and abuse.” The agency said this was likely due to caseworkers’ high workloads, noting that the department “must address persistent staff vacancies.”
“In order to comprehensively evaluate the risks posed to children, workloads must be manageable for caseworkers,” the agency wrote. “Persistent staffing vacancies create higher workloads and a need to triage cases to meet minimum required expectations and to address the cases in which children are at the highest and most immediate risk.”
The agency recommended that OCFS conduct a comprehensive examination of caseworker vacancies, and determine new strategies to recruit and retain staff.
Jaden Harding
Jaden Harding was shaken to death by his father, Ronald Harding, when he was just 6 weeks old.
The 65-page OPEGA report on the case lays out the lengthy history Harding’s mother, Kayla Hartley, had with Maine’s child welfare agency dating to 2014 and related to her other children. This history included errors OPEGA determined the agency made around properly assessing all the people who spent time in Hartley’s home.
However, the report notes that Ronald Harding “did not appear, from our review, to have presented earlier actionable safety threats to Jaden.”
The OCFS investigation into Hartley was closed before she became pregnant with Jaden. And while OPEGA again found OCFS did not conduct a criminal background check on Harding, it also noted that such a search wouldn’t have found anything. But it did identify an old, screened-out report to OCFS that mentioned Harding. (OPEGA did not describe the content of this report or how old it was.)
If it had been identified while Jaden was alive, OPEGA notes it likely would have prompted a caseworker interview with Harding, but the watchdog ultimately concluded the information in the report wouldn’t have “been sufficient for the Department to intervene in any way with the family.”
In its report, OPEGA noted that “OCFS should develop a process and standard for identifying which families’ CPS histories should be subject to a more comprehensive review,” and should ensure that staff have the time and resources to conduct such reviews.
The agency again pointed to caseworkers’ high workloads as a problem, and reiterated the need for caseworkers to have a comprehensive understanding of a given household’s structure.
“OCFS should consider revising its investigations process and related checklists to require caseworkers to confirm a family’s living arrangements, and all household members have been identified when nearing the end of an investigation,” the agency wrote.
OPEGA also pointed to a need to better identify and provide necessary services; improve information sharing between law enforcement agencies, the courts and OCFS; and for OCFS management to provide more feedback to supervisors and caseworkers.
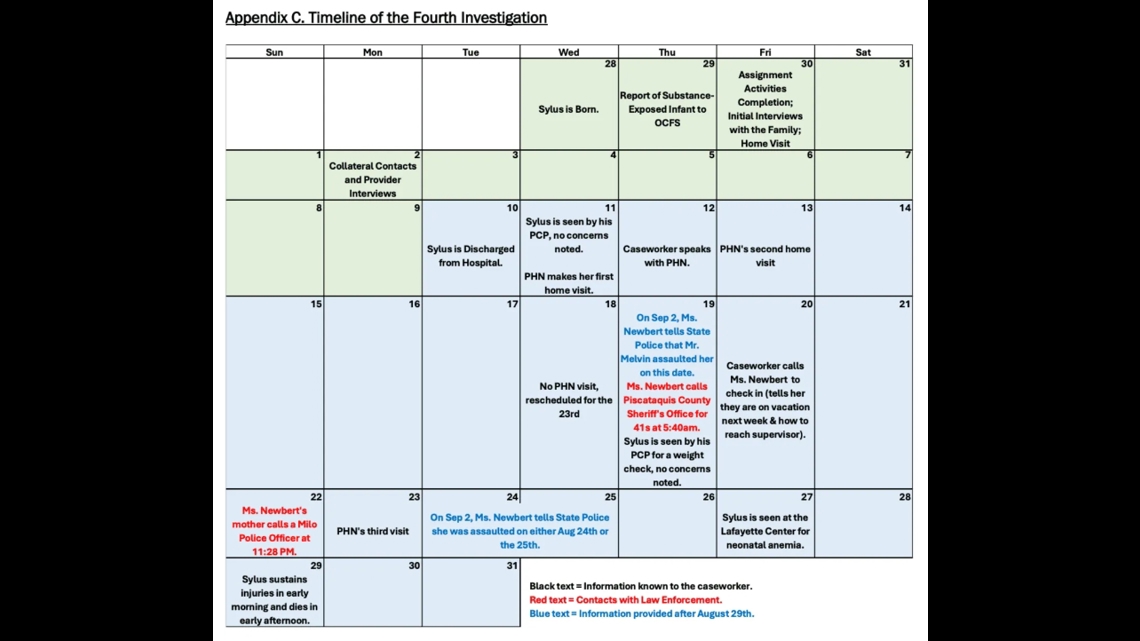
Sylus Melvin
On Aug. 29, 2021, Reginald Melvin killed his son, Sylus, who had been born substance-exposed a month prior.
OPEGA concluded that casework during the boy’s short life was “sound” and the caseworker was “thorough.” The family had a long history of OCFS involvement before his birth, involving substance abuse and domestic violence.
In the month Sylus was alive, a caseworker and public health nurse were checking in with the family and reported no concerns. An Aug. 19 family visit to the doctor did not raise any red flags.
Sylus’ mother and grandmother reported that Reginald Melvin used illicit drugs and was physically abusive to Sylus’ mother and made violent threats, and said they notified OCFS and law enforcement. OPEGA investigated the claims and determined caseworkers did not know about the issues until after Sylus’ death, but encountered difficulty because of missing phone records.

OPEGA noted in its report that though safety planning practice has changed since this case, “safety plans remain an area of uncertainty for some caseworkers today,” and recommended that the office continue to clarify what constitutes a safety plan.
The report recommended that the office involve caseworkers and supervisors when drafting a public memo that follows a child’s death, noting that in Melvin’s case there were inaccuracies: “As this may be the only public accounting of what occurred in the case (other than related prosecution), it is vitally important that the information in those memos is accurate.”
The agency also recommended that the office hold onto relevant call logs and texts when there is a child fatality; and noted again the need for better communication and information-sharing between law enforcement and OCFS.
‘Significant restructuring’
In a 2022 report on the child welfare system, OPEGA described the “misconception” that “adverse outcomes are the fault of caseworker error of flawed processes.”
“Adverse outcomes occur for complex reasons and can occur despite quality staff and processes in place,” the agency wrote.
Maine’s child welfare office, like many across the country, has struggled with too few workers handling large caseloads and a limited budget.
The Department of Heath and Human Services has made a number of changes in recent years, including a reorganization announced in January, and has been flooded with recommendations and findings from government and private sector organizations.
“There has been significant restructuring within the Office of Child and Family Services’ central office, positions added in the districts (training supervisors, for example), and efforts to increase retention of staff,” said child welfare ombudsman Christine Alberi in an email. “I think most importantly during 2024 there has been a significant shift in philosophy, and a willingness to acknowledge and work proactively on some of the longstanding issues DHHS has.”
A DHHS spokesperson, Lindsay Hammes, said OCFS has “dedicated significant resources to strengthening child welfare and to working with the legislature to look holistically at the child welfare system and identify areas for improvement.”
She said the department is collaborating with other partners to strengthen “supportive services for families that are targeted at preventing the need for child protective involvement in the first place.”
She mentioned the Child Safety and Family Well-Being Plan and the Be There for ME programs as examples.
‘A delicate balance’
In its report on Maddox Williams, OPEGA noted that the public’s understanding of how the child welfare system operates is limited.
“Throughout our review of the child protective services system, OPEGA has observed a disconnect between what the public expects the system is (or should be) doing and what the system is actually doing or capable of doing (as informed by law and policy),” the agency wrote. “The field of child welfare exists as an array of competing interests that strike a delicate balance. Not everyone will agree as to what best serves a child, but it is a topic worthy of further discussion.”
The public’s lack of understanding stems in part from the secrecy around most child welfare proceedings: Only the most extreme cases move from confidential files to the public record. Child welfare advocates have argued that more transparency is needed to ensure confidentiality rules are protecting children and their families, not shielding the government from scrutiny.
While the reports highlight the most horrifying of possible outcomes in child welfare cases, they don’t address the other end: when children are removed from their parents unnecessarily.
Maine in recent years has bucked the national trend in child removals: It was one of just four states that grew its foster care population between 2018 and 2022, increasing the number of children in state care by 24 percent, second only to Illinois, according to the most recent federal data.
And yet removing more kids from their families hasn’t lowered rates of child abuse: The data shows that Maine is one of just seven states with more instances of child maltreatment over those same five years. Maine’s rate of maltreatment increased by 9 percent from 2018 to 2022, second only to Nevada’s 14.5 percent increase.
Some advocates suggest the money spent on child welfare investigations would be better spent on supporting families living in poverty, which they argue is the real driver of child abuse and neglect.
One 2021 study, for example, found that child fatalities decreased by nearly 8 percent for every additional $1,000 states spent on benefit programs per person living in poverty. Another 2017 study found that child neglect reports decreased nearly 10 percent for every dollar added to the minimum wage.
After the hearing, the House chair of the oversight committee Rep. Jessica Fay, D-Raymond, told The Monitor her main takeaway from the reports was how intertwined child welfare was with substance abuse and domestic violence.
In recent years, more than half of all Maine child removals involved substance abuse, according to the state’s annual child welfare report.
“I think we often look at things as silos,” Fay said. “And this has shown us how interconnected all of these issues really are.”
This story was originally published by The Maine Monitor, a nonprofit and nonpartisan news organization. To get regular coverage from the Monitor, sign up for a free Monitor newsletter here.