
WASHINGTON (NEWS CENTER) — A federal audit report released Thursday found Maine's Department of Health & Human Services (Maine DHHS) to be in non-compliance with several federal and state requirements concerning critical incidents that involve developmentally disabled Medicaid beneficiaries.
The audit, conducted by the U.S. Department of Health & Human Services (HHS) from January 2013 through June 2015, was part of a series of reviews in several states focused primarily on the reporting and monitoring of deaths and cases of abuse of residents with developmental disabilities being cared for by community-based providers.
Medical records and critical incident reports from the 30-month period reviewed by HHS indicate Maine did not comply with requirements for reporting and monitoring critical incidents and therefore, in doing so, "failed to demonstrate that it has a system to ensure the health, welfare, and safety of the 2,640 Medicaid beneficiaries with developmental disabilities covered by the Medicaid waiver."
► DHHS argues federal report findings are incomplete, outdated
| Community-based providers failing to report all critical incidents |
Federal waivers allow states to furnish an array of living options so beneficiaries can live in community settings and avoid institutionalization; however, in turn, the states are required to implement an incident reporting system to protect the health and welfare of the beneficiaries.
Community-based providers in Maine are required to report to the state all critical incidents involving Medicaid beneficiaries with developmental disabilities. Such incidents include physical and sexual abuse, neglect, serious illness, injury or death.
According to the report, HHS determined Maine providers reported just 66 percent of the nearly 2,300 critical incidents. Providers told federal agency officials that staff turnover and clerical errors contributed to the unreported incidents, yet state officials were unable to provide an explanation as to why it wasn't ensuring providers reported all critical incidents.
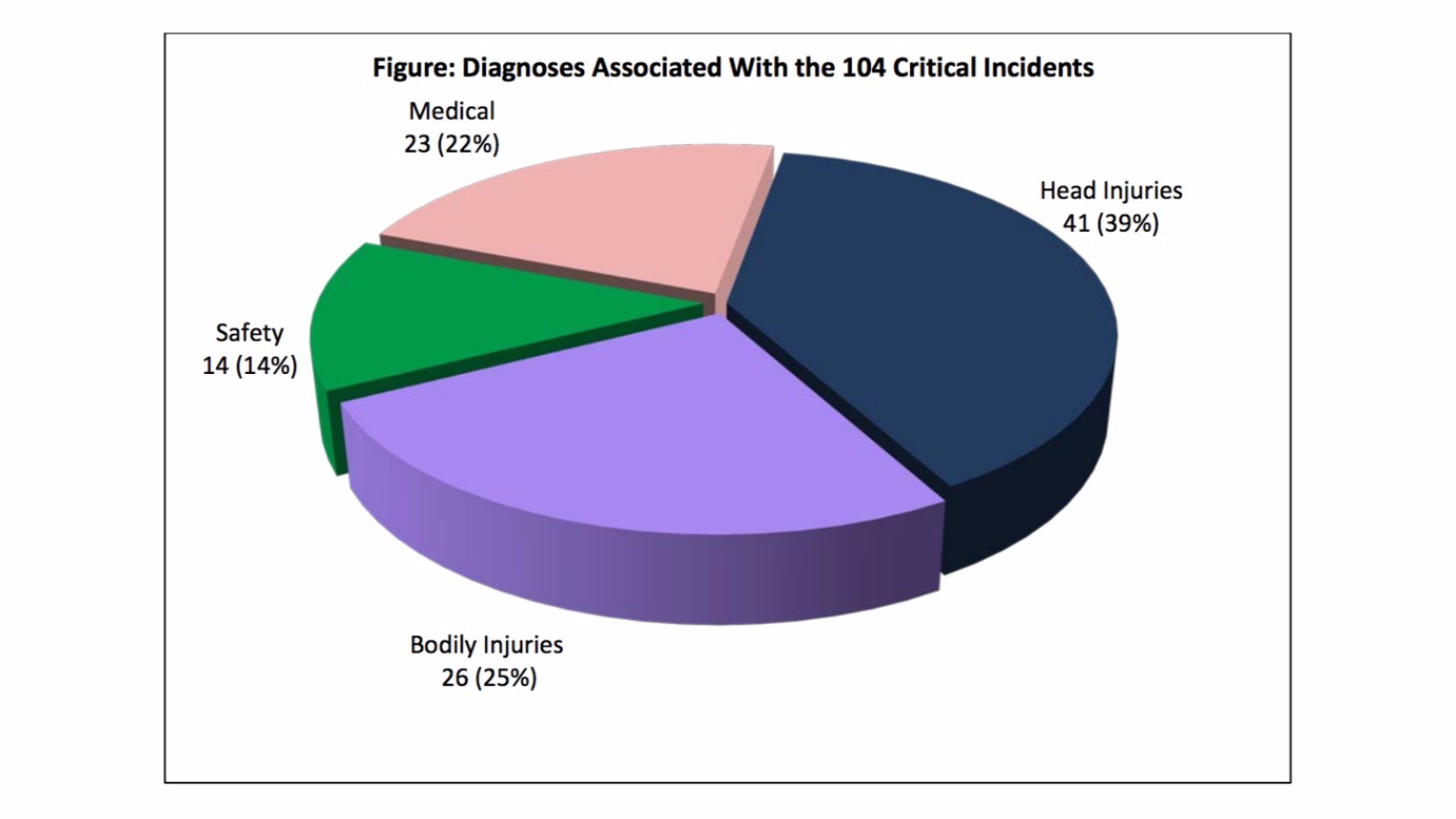
Of the 769 unreported incidents, the feds selected 104 "high-risk" critical incidents — later confirmed after review by state agency officials as reportable incidents — and examined them separately. One such case provided as an example of an unreported incident claims a beneficiary suffered a "jagged" laceration that required sutures to close the wound. Records show, according to HHS, the provider's staff stated the cause of the injury was unknown and the beneficiary could not provide a history of the injury.
Federal officials state that, because the injury met Maine DHHS' definition of a "critical incident," it should have been reported by the community-based provider.
| Failing to ensure providers reported all deaths |
According to the report, Maine DHHS did not investigate any of the 133 beneficiary deaths during the feds' 30-month audit period, nor did law enforcement open up any investigations into the 133 deaths. Additionally, the report found no evidence was provided to a committee tasked with identifying potential trends.
Maine DHHS told the federal inspector general's office that the Mortality Review Committee reviewed 54 of the 133 beneficiary deaths, but HHS claims documentation provided by the state did not detail what the reviews entailed or the outcome, including potential corrective action. The state medical examiner's office reviewed 13 of the 133 beneficiary deaths, HHS said, but did not receive referrals from or share the results of the reviews with Maine DHHS.
| Failing to investigate and immediately report incidents |
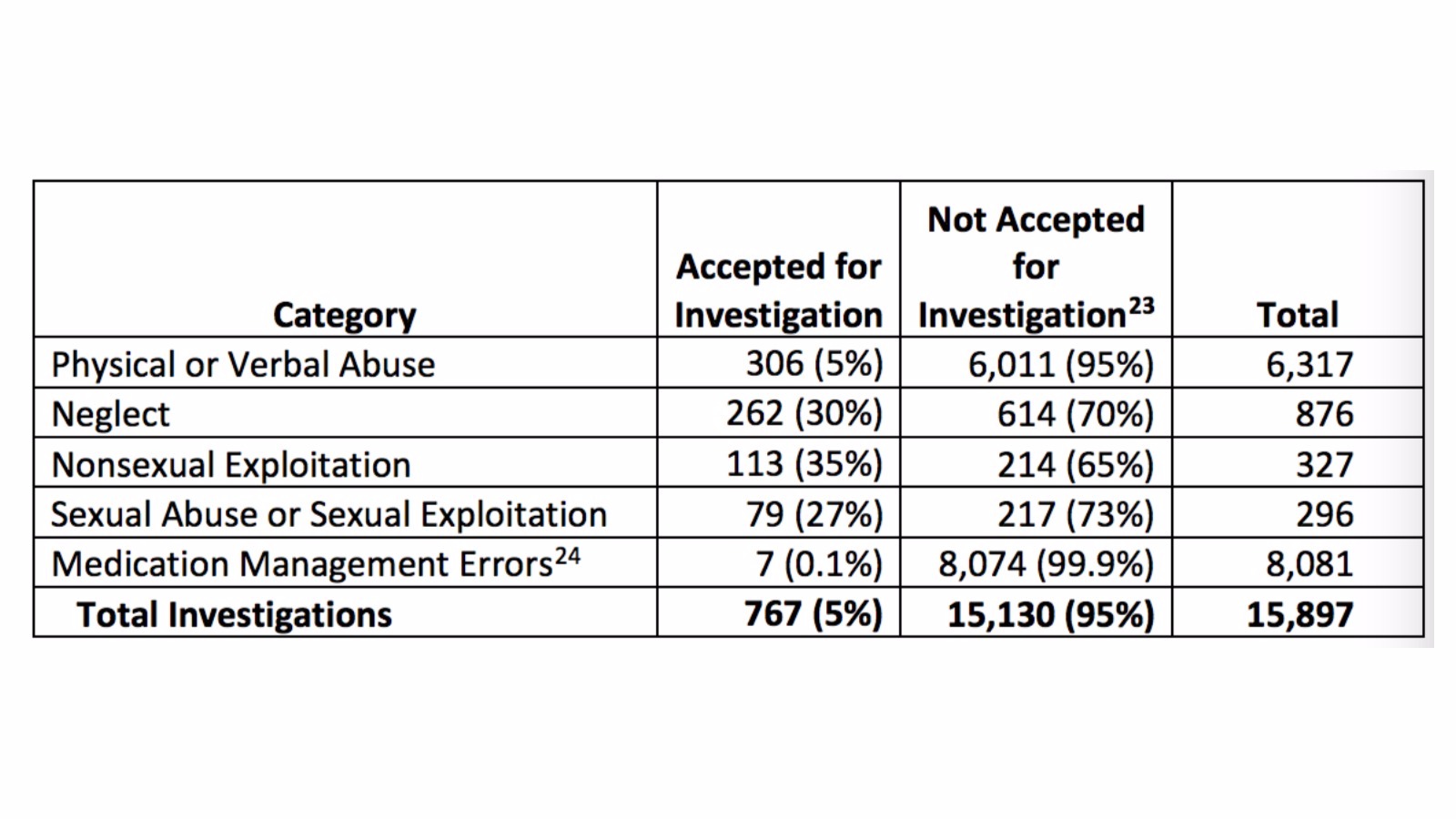
The federal report also revealed just 767 — 5 percent — of the nearly 16,000 critical incidents involving potential abuse or neglect dealt with by Maine DHHS between January 2013 and June 2015 were accepted for investigation.
An example of an uninvestigated death provided in the report by federal officials detailed a female beneficiary who drowned while unattended in a bathtub.
Citing the critical incident report, it states that a staff person was physically assisting the beneficiary and the beneficiary "pushed" the staff person away. After leaving for five minutes to give the beneficiary time alone, the staff person returned to check on the beneficiary and was again "pushed away." Shortly after leaving the bathroom a second time, she heard a "thud" and immediately returned to find the beneficiary with her face under water and her arm over the side of the tub.
Emergency personnel were contacted but attempts to revive the person were unsuccessful. A subsequent review by the state medical examiner's office determined the cause of death as accidental drowning.
The death was never investigated by the state, the federal inspector general's office said, therefore squandering an opportunity to identify any preventable causes, such as the lack of bathing safety or adequate beneficiary monitoring.
* * * * *
In summary, the report found Maine DHHS failed to ensure the following…
- Ensure that community-based providers reported all critical incidents to the state
- Ensure that community-based providers conducted reviews of all critical incidents involving serious injuries, dangerous situations or suicidal acts and submitted their findings within 30 days
- Appropriately report all restraint usage and rights violations to Disability Rights Maine
- Review and analyze data on all critical incidents
- Investigate and report immediately to the appropriate district attorney's office or law enforcement all critical incidents involving suspected abuse, neglect or exploitation
- Ensure that all beneficiary deaths were appropriately reported, analyzed, investigated and reported to law enforcement or the state medical examiner's office
Federal officials said Maine DHHS agreed or partially agreed with seven of the report's recommendations and with four of their six findings. The state did not agree with the assertions that it, one, had failed to ensure community-based providers reported all critical incidents and, two, had not investigated or reported critical incidents to the appropriate authorities, but federal officials said they stood by their findings.
The full report can be found below:
Maine Handling of Dev Disabled a-01!16!00001 by NEWSCENTER26 on Scribd